

In late May, Swiss BCI startup ABILITY Neurotech received approval to begin its first clinical study. The headline could easily have gone under the radar, crowded out by larger US funding rounds and Chinese regulatory milestones. But ABILITY is no small interface project. The ECoG developer spent ten years inside the Wyss Center developing and de-risking its platform. Now, after tens of millions of dollars in investment, its optical data-link architecture will be tested in a cohort of ALS patients.
The study, taking place at UMC Utrecht and TU Graz, will test the safety profile of ABILITY’s implantable BCI and evaluate whether the system can support communication, computer control, and speech in a home setting. The company builds on the thesis that data transmission is the main bottleneck for real-world BCI deployment. While ECoG traditionally offers lower resolution than intracortical approaches, ABILITY believes that wider coverage combined with a high-throughput optical link can create a more sustainable data stream than its more invasive cousins.
ABILITY Neurotech emerged about a year ago after spending ten years as an R&D project inside the Wyss Center. With investment into the platform reaching roughly $50 million, the project moved into commercial form in March of 2025. Rotem Kopel, CEO of ABILITY, sees that origin story as a key strength. “We really had a different start because the Wyss Center is unique,” she says.

The Wyss Center, located in Geneva, Switzerland, was not built as a conventional academic neuroscience institute. Founded in 2014 by philanthropist Hansjörg Wyss, the center was designed to sit between neuroscience, engineering, clinical work, and translation. Hansjörg Wyss brought in John Donoghue as its first director, one of the central figures in the earlier BrainGate generation of implantable BCI.
ABILITY emerged after spending years on technical development and preclinical work, benefiting from accumulated IP, clinical relationships, and expertise around what a BCI should optimize. This allowed the startup to essentially derisk the device from day one. “The beginning of the project was to rethink the device, starting from a blank page and really analyzing the components or the blocks that every BCI should have,” says Kopel.
“You cannot innovate the electrodes, the implants, the communication, the materials, the amount of data you transmit, the decoding, and the system itself,” Kopel says. “You have to ask what the critical parts are that would actually create a product.” For ABILITY, the answer is built around data transmission, external decoding, and clinical usability.
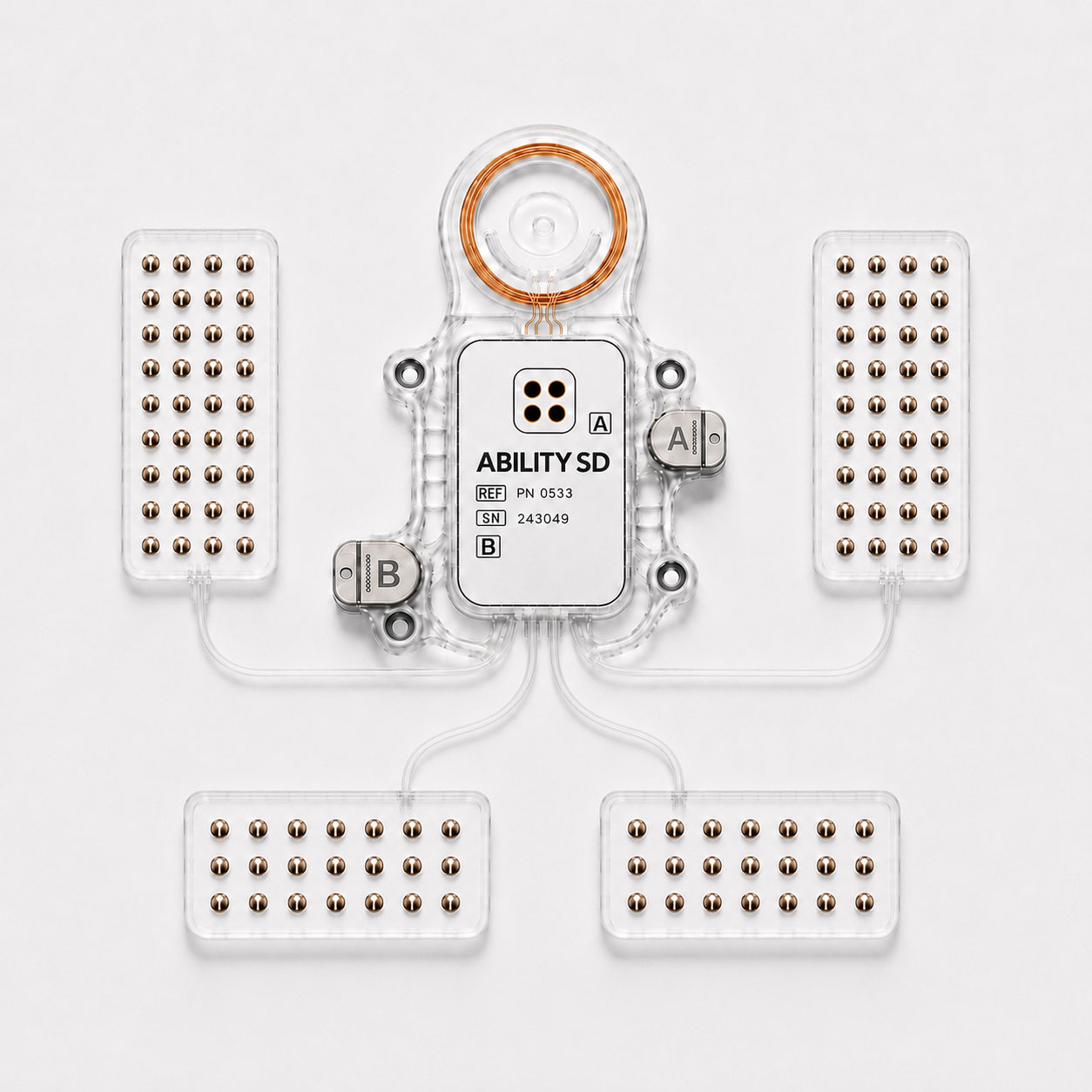
ABILITY has developed an ECoG-based BCI around the belief that in real-world deployment, the bottleneck is not just the interface’s resolution but how much neural data can consistently be transferred out of the body for decoding. ABILITY’s implant incorporates 128 channels, records from the cortical surface without penetrating tissue, and is designed to preserve a broad neural signal for external processing.
The main differentiator compared to the competitors is an optical link. The system uses a transcutaneous laser to stream raw neural data out of the body at up to 50 Mb/s. Kopel contrasts that with Bluetooth-class wireless transmission of competing interfaces. “Every time you transmit one bit via Bluetooth, we transmit 50 at the same time,” she says.
The system’s trade-off sits in the sensing layer. Intracortical systems can record more precise local activity from smaller brain regions. ABILITY’s ECoG-based approach records with lower spatial resolution, but across broader cortical networks.
“We went with an ECoG that has very wide coverage, with the understanding that our brain is mostly networks,” says Kopel. That is especially relevant for speech, one of ABILITY’s first targeted use cases. “Our wide coverage of the brain means we do not just record areas that relate to motor pronunciation, but also language.”
Speech is one of the clearest tests for invasive BCI, restoring a natural communication channel for those who have lost that ability due to neurodegenerative disease. In 2023, Stanford researchers decoded attempted speech from a participant with ALS at 62 words per minute using intracortical microelectrode arrays. That same year, UCSF’s Edward Chang group reached a median of 78 words per minute using high-density surface recordings, inching closer to the ±140 words per minute of natural speech.
Yet the field still lacks a clear deployment strategy. The best demonstrations have been in very small numbers of patients, often in controlled research settings. And as such, the companies exploring speech decoding in patients face a range of unresolved questions. Can models transfer across patients? How much training does each person need? How often do systems need recalibration, and how does performance change with disease progression, plasticity, and implant ageing? “We don’t yet have a full playbook of how to do it on a wider population,” says Kopel.
One of ABILITY’s US competitors, Paradromics, has been explicit that high-performance communication BCI requires high-data-rate intracortical recording, with its Connexus system built around penetrating microwire electrodes. Kopel does not dispute that intracortical systems capture more precise local signals, but argues that precision also brings trade-offs around placement, stability, and coverage. “There is no question about the fact that you get a better signal with intracortical,” she says. “But there is a price to pay for that precision.”
The surface-recording argument is supported by the UCSF work, which showed that high-performance speech decoding can be achieved without penetrating electrodes. Kopel points to that work as evidence against the claim that ECoG cannot provide enough bandwidth for speech. “I would challenge that statement,” she says. “Definitely, there is clinical work that presents something that contradicts it.”
Late last month, ABILITY received approval to begin its first chronic implantation study in people with ALS. The study will principally evaluate safety, while also looking at communication through cursor and computer control, software interaction, and speech decoding. The trial is being built through the INTRECOM consortium, which includes UMC Utrecht, TU Graz, ABILITY Neurotech, and German BCI firm CorTec.
For ABILITY, an equally important endpoint is real-world deployability and home use. Kopel highlights just how far the field has come since the earlier BCI research systems built around bulky lab infrastructure. “[In the past] you had to come to the lab, and there were three PhDs. One is connecting it and controlling it. Another one is maintaining the position of the signal, analyzing it, and training the patient.” She continues, “For us, the real goal would not be scores on a graph, but for the patient to actually use it.”
It is hard to ignore the regional significance of ABILITY’s study. In China, BCI has moved into a national strategy. In the US, the field is shaped by private capital and the gravitational effect of Musk’s Neuralink and Altman’s Merge Labs, each raising hundreds of millions at billion-dollar valuations. Europe has impressive technical and clinical nodes, but the field does not benefit from the same level of centralized strategy or venture intensity.
And yet, Europe is now home to a range of strong BCI startups. ABILITY sits in a category featuring INBRAIN in Spain, CorTec in Germany, and Swiss neighbour Neurosoft Bioelectronics. Still, Kopel argues that the achievements of individual companies and labs are not enough on their own. “To just keep on doing what we did up until now, we would never be in the race."
Her concern is not only capital. It is also where the clinical work and data will accumulate in the near future. If the next generation of invasive BCI studies is concentrated in the US and China, Europe risks losing more than company formation and economic returns. “We would miss the clinical work, we would miss developing the labs, we would miss the data,” Kopel says. “Combining AI with the data that companies like ours will extract is mind-blowing. Not being there for this revolution is going to be something we would regret deeply in Europe.”
Kopel sees several possible routes for Europe, from EU-level grants to private capital and regional public investment tied to facilities, trials, and expertise. “But it would not happen because Frank [CorTec], Carolina [INBRAIN], Nicolas [Neurosoft] and I are pitching,” she says. “It’s not enough.” And so, ABILITY’s study will not elevate the EU to the level of China or the US. But perhaps, by showing what is possible when capital, expertise and resources align, ABILITY can spark a conversation in Brussels around a more coordinated European BCI push.
.svg)










